Food is the basic requirement of every living being. Good food is a human weakness. People go to hotels and restaurant to have food of their taste; and hotels and restaurants are known for the kind of the food they serve and more so; the way they serve. There is some difference between the food we get in hotel and hospitals. In hospital people do not go to have food, but if the hospital caters to the need of the patient, visitors and hospital staff in the same manner, in which it is served in good hotels, it adds value to the services. Good food is an important determining factor in delighting the patient, visitors and hospital staff.
Dietary service is an important department of modern hospital. In view of growing medical tourism, the hospitals are supposed to develop good dietary services, in the pattern of the hotel industry, as it is medical care combined with tourism, so due care is to be given while planning the dietary services of the hospitals, so that visitors do not have to go to hotel for food.
The food services department may be owned by the hospital or it may be on contractual basis or what is popularly known as out sourcing or public private partnership (PPP). The students are advised to consult the chapter on contracting in health care in the same book. In outsourcing also, it will depend upon the extent of out sourcing, whether partially or fully, whichever kind of dietary service is available it is grouped into two basic categories.
Food is prepared and processed or cooked in the hospital’s main kitchen and food trays are planned, prepared and served and conveyed to the hospital floor by trolleys. There are certain advantage and disadvantage of the service:
Food is prepared, processed and cooked in main kitchen of the hospital and transported in bulk to the ward pantry or directly to the patient bed side for serving. This system also has certain advantages and disadvantages.
In this modern era, the image of hospital is changing and it is important to understand the reason for increasing importance of food safety in hospitals. The traditional role of a hospital was equated to providing curative services only.7. The role of hospitals underwent a paradigm shift in the past 50 years. In the present time WHO encourages hospitals to think away from disease- and illness-oriented care to towards more holistic healthcare, as health-promoting hospitals (HPH). As per this approach, the hospitals are not just seen as curative centres but also as a place that actually promotes healthful living. Nutrition/dietary/catering services are important aspects of HPH concept. In a health-promoting hospital, food safety is a vital concern. Food safety in a hospital requires special attention so as to minimise the hazard of foodborne diseases. Hospitals should take a lead in providing safe food to patients, hospital employees and visitors. The health-promotion approach also necessitates that the hygiene of EE in hospital premises as well as the hospital kitchen is maintained at an optimal level. So, in the present context, the concept of HPH and food safety can be integrated to ensure good quality of services.
Hospitals, as a setting and as a place of work, engages cadre of employees and caters to thousands of patients and their relatives. Food service facilities are used by hospital staff and patients as well as their visitors. For the admitted patients of the wards, provision of good quality and safe food is responsibility of the dietetics department. Patients are prescribed special diets as per the disease suffered by them (renal/ diabetic/hypertension diet). Good nutrition can promote speedy recovery. These groups of patients are also exposed to the food available outside hospital premises through their visitors.
On a typical day a patient comes (alone or with attendants) to a hospital and gets registered. From here he is directed to one of the departments (outpatient department (OPD)/inpatient department (IPD)/diagnostic services/ blood bank/pharmacy, etc.). All the processes in hospital take time. They need to start early in the morning from their homes in remote areas to reach hospitals in time. Patients and their relatives may not get enough time to take a proper meal from home. He has two options available-one is to carry his food from home and the other is to procure food available in the hospital premises. In most of the cases, latter is a preferred choice due to sheer inconvenience of carrying cooked food. The same holds good for the people accompanying the patients.
The employees of a hospital, like anywhere else, often spend as much as 60% of their working hours in their place of work. They are also exposed to all the eating options available inside hospital premises. The food options made available to them by employers can greatly impact upon their health. The good health of medical and paramedical professionals is also important for setting an example to the local communities within which they are based. Hence, canteens/EE play a very important part of hospital support services.
| Patient’s | Non-Patient’s |
| Ward Patient’s | Relatives/visitors of patient’s |
| OPD Patient’s | Employee (permanent, contractual) |
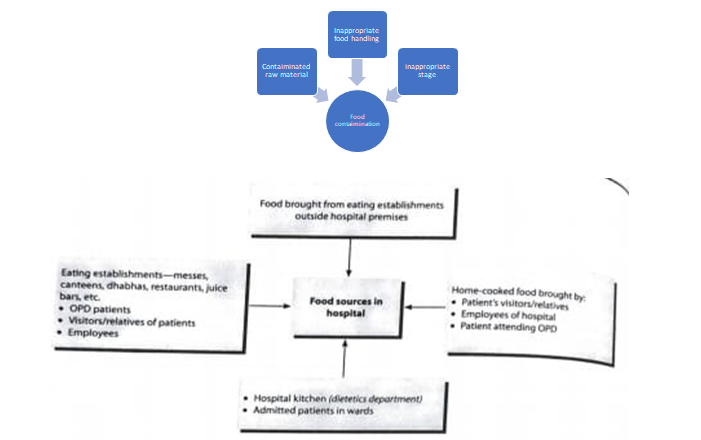
Food safety in hospital is a daily challenge. Large volumes of food are prepared/brought in by contractors, kept warm at safe temperatures, distributed though long corridors and served to a large number of patients by many hands. Food contamination can occur at any point from its journey to procurement of raw material to it being served to the client. Unhygienic raw material can make the food unsafe by cross contamination with cooked food or during inadequate cooking. Improper handling of food permits contamination, existence and growth of infectious organisms. The common errors in food handling are contamination by food handlers during transportation and/or serving of food through unclean utensils. Improper storage (storing food at room temperature) or inadequate refrigeration, inadequate reheating can also lead to food contamination. This will depend on the source of food. Though desirable as of now, hospitals can do little to monitor or control the quality of food brought in the hospital by patients, relatives or employees.
The next sources of food are the EEs inside hospital premises. This is commonly used by the OPD patients, their attendants and the hospital staff. Food may also be procured from EEs outside hospital premises brought for consumption in the hospital. In addition, the hospital dietary services department caters to the patients and the staff based on their specific requirements as per the disease condition. The main kitchen in a hospital daily prepares food for distribution among patients as well for employees. This may be distributed in the form of traditional meal delivery system in trolleys or room service system in hospital kitchen. Let us discuss here the food safety aspects in respect of hospital kitchen. Safety of food can be ensured through good hygiene practices (GHP), good manufacturing practices (GMP), ISO 22000 certification, adaptation of hazard analysis and critical control points (HACCP) principles, etc.
For every hospital kitchen there should be a specific food safety policy. It is proposed that a
Multidisciplinary food safety team’ should be constituted in a hospital to make the food safety plan for the hospital and ensure implementation of the plan. Various functions of the food safety team suggested are given below:
It is also recommended that there should be a food safety officer (trained in food safety) for the hospital. The proposed functions of food safety officer are given below:
Quality and quantity of raw material and finished products has to be maintained up to a certain standard. Quality standards need to be maintained while procuring raw food items. Perishable items such as milk, bread, non vegetarian items, vegetables and fruits as well as non-perishable food items like wheat and other cereal flour, rice, pulses, dry ‘masalas, etc. are usually purchased on tender basis. It should be kept in mind that good government agencies like Verka, Hafed, Britannia, etc. may be roped in for the supply of milk, cheese, bread, rice, etc. since they have their own quality standards. Regarding non vegetarian food items, vegetables and fruits, lowest tender bids are usually taken in by the administration, but a hawk’s eye has to be kept on the quality like freshness of fruits and vegetables and non vegetarian items. Fulfilment of benchmarks kept for quality analysis is a must.
Usually these are not procured on daily basis; let us say, twice a week. A team comprising of a nutrition expert, store officer and member of hospital administration is usually there along with the vendor when these items are received. All gunny bags containing fruits and vegetables are emptied and the kitchen working staff sees each and every piece for its freshness. Then these are again repacked and weighed on an electronic weighting scale to record the final weight after taking out the wastage. This whole task takes almost 1½ hour. Then the fruits and vegetables are transferred to the cold storage room where they are again weighed so that they tally with the initial weight. This is done to check any pilfer age on the way!
Procurement of nonvegetarian items in the hospital is thrice a week, e.g. eggs, chicken, fish. Since mutton being red meat, it is best avoided in hospital’s menu. The quality of fish becomes dicey in summer months; hence it is avoided in hospitals.
Eggs come in numbers and are checked randomly for quality by putting them in water. If an egg floats, then its quality is under suspicion since it is a sign of a rotten egg. Storage of eggs is in cold room. Chicken is checked for its quality by visual analogue scale; seeing the toughness of skin that it is clean from inside, free from any liver and other fillers. Quantity is weighed after ensuring that there is no water in the chicken packets, since these are kept in cold storage after being slaughtered; therefore thawing may add some water to the packets. If it is so, some weight is subtracted. Secondly, the necks have not to be more than 2 inches, since it is just a waste and adds to weight. If so, again some weight is subtracted after giving warning for the next supply. It is kept in cold storage.
Milk is a daily-supply item. Milk supply should be from a genuine government agency. It is best to receive milk in packed packets for industries, e.g. a 5-1 packet. This way, the hygiene part is ensured. Receiving milk in ‘dampoos’ or big drums might not be that hygienic, since it involves manual handling. Same way, it is best to procure cottage cheese and tofu in packets like ‘Verka’ cheese supply. The manufacturing date and ‘best before should be taken care of. All these milk products are stored in separate cold storage and not where nonvegetarian items are stored.
Ration items like cereal grains, pulses, masalas, etc. are checked by a team consisting of the head of the dietetics department, store officers, officials from administrative department along with the vendor. These are checked for grain size, colour, unwanted polishing and any foreign material in the grains. When the quality is approved, these are weighed and stored in dry ration storage area.
Walk-in cold stores and deep freezers are a boon, since the things can be stalked and reached easily and also can be accounted for. Walk-in storage also has enough capacity for storing various food items. For dry ration storage, the store should be well-ventilated and lighted, free from dampness and the pesticide and insecticide treatment should be carried periodically.
Pilferage is the biggest issue in food industry and that too when the workers employed are from lower social strata. Pilferage at all the stages, whether it is dry ration or cooked food has to be controlled since if not taken care, will make all the previous exercises of quality and quantity control futile.
This should be done by tasting the normal meal as well as therapeutic diets and feeds (hepatic, renal, anti obesity, diabetic, burn feeds, etc.) by a team of nutrition experts. The trolleys should be allowed to leave the kitchen area only when the team is satisfied.
The meals and feed portions should be periodically standardised to ensure correct calculation and delivery of nutrients. The measuring units for meal, especially feed preparations, have to be correctly calibrated and preparation needs to be closely monitored to ensure proper intake of macro as well as micronutrients by the patients. Kitchen layout should be glass enclosure for preparing all therapeutic feeds so that the counter for feeds remains separate and can be monitored from outside.
In fact, the most crucial and important resource is HR management. There is always a mix of regular and contractual workers. A lot of responsibility is required for a team of healthy happy working force. The officers have to take care about their being disease and germ free, since they are working in a very vulnerable area of the hospital, i.e. food preparation, handling and distribution. So it calls for regular medical check-ups for any allergies, skin disease, tuberculosis, etc. In addition to their blood and urine tests, nail, nose and sputum swabs are also tested for any infection. The workers found to be having any kind of infection are given a break along with a course of medication. Before joining, they have to ensure their fitness through medical tests.
To ensure good health of workers, the working conditions have to be apt. Daily monitoring of clean uniforms, shaved beards, nails cut neatly, regular hand wash when they enter kitchen, prepare meal, handle the food and come back after distribution has to be ensured by the dietetics staff. Clean aprons with a pocket for keeping paper towels, disposable caps and gloves are an essential part of their attire. Heavy fines should be imposed for defaulters. To facilitate workers health and hygiene as well as comfortable working conditions, chimney having appropriate suction capacity should be installed. Adequate number of porcelain/stainless steel washbasins should be there, having soap dispensers installed to wash hands, and neat and clean towel to dry hands. Hand dryers would be a better idea along with paper towels.
Separate sinks should be provided for washing raw food and a separate area for washing pots and pans. Conveyor belt for preparing chapatti makes it convenient for workers to toll out chapattis. Bulk cookers are a convenient option to cook food for say about 1000-1200 patients.
It becomes mandatory to clean food preparation areas and equipment’s. The staff should be given dear instructions about what needs to be cleaned, how often and the way to do it. It should be ensured that all repairs are made as early as possible by instructing the staff to report all breakdowns immediately. Food trolleys are being used to carry cooked food to various wards. Food trolleys, if used in hospital for delivering food to patients, should be dedicated for this purpose and not used to carry anything else. Time required for transportation should be kept to minimum to avoid microbial proliferation. The trolleys have to be kept covered during their journey from kitchen to the wards. Handling of cooked food should be minimal. Food handlers must use disposable gloves while distributing food in the wards after ensuring hand hygiene. All surplus and unused food should be discarded to animal houses.
Staying healthy also calls for well-ventilated kitchen with proper air circulation and cooling system so that workers remain perspiration-free in long Indian summer months. The kitchen area should not be a thorough fare. Either there should be card system that only swipe of card at the door allows entry to officers and workers of the kitchen department or a guard should be sitting at the entrance prohibiting any patient or an outsider to walk in. Separate route and a room for catering to indoor diet grievances should be there, which is not enrooted through the food preparation area. This way, seepage of infection in the food area would be minimised.
Since the cooks and bearers are the people who will have direct contact with machines, their work safety should be one of the priorities. Working with machines has its own risk of accidents like getting injured or hurt; therefore, workers should have thorough knowledge, training to work on the machine and strict instructions about the dangers of mishandling or being careless while handling any machine related work. For example, in our hospital kitchen twice the workers got injured and nearly lost their hands while working on chapatti making machine and slicer. One worker’s hand came beneath the dough roller and was compressed since he tried to manually pick up a dough ball just before it was being getting rolled! The other one was talking and his hand nearly got sliced in a slicer!
The department should have close proximity to the materials management department. It must have easy accessibility to the unloading dock and for vertical transportation system. The cafeteria and dining hall should be close to the food preparation room.
As a general rule 50 sq. feet per bed for 50 bedded hospital and 15 sq. feet per bed in 500 bedded hospitals. In UK 8-10 sq. feet per bed of space is recommended.
The determining factors for type of dietary services and size of the department can be enumerated as follows:
The various facilities of dietary services should be grouped in one area for smooth functioning of the department:
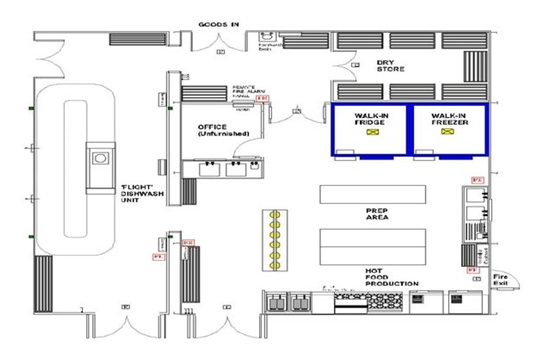
It should be accessible to roads where the unloading of trucks can take place without disturbing the hospital functions and causing noise pollution. The outside door should be 5 feet wide. The receiving area is equipped with a platform scale for weighing. The storage area should be divided into a dry storage area and storage area for perishable items like vegetable. The storage area should be near to the preparation area. Separate storage area should be for linen, equipment’s, dishes and LPG Gas cylinder. Refrigerated storage area for the items to be stored in cold temperature. Thus, the storage areas can be divided as:
a. Walk in refrigerators
b. Reach in refrigerators
c. Under counter reach in refrigerator
Preparation area can be divided into:
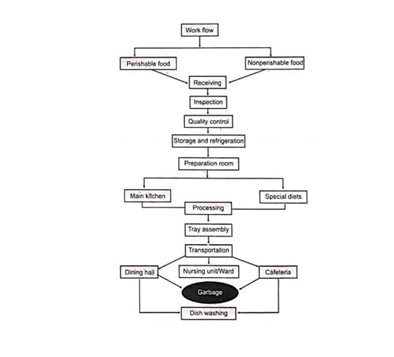
The size of kitchen will depend upon the food programs and menus. The main kitchen gets supplies from the stores, refrigerators and preparation room and from there it issues to the serving area. It is also in direct communication with the dish washing area and also to the intramural transport entry points.
Generally, little alteration is required in addition to the normal diet and so minor equipment’s will be added to the list of special diet area. It is conveniently located next to the dietician’s room to have better supervision and control.
In paediatric wards, where the baby foods are prepared for new born, a formula room is required. It should be adjacent to the nursery.
In hospitals having decentralized dietary services, the serving room is not required. The serving room receives food in bulk from main kitchen and trays are prepared and issued to the ward floor either through conveyer belts or trolleys.
The cafeteria and dining hall should be adjacent to the kitchen. Attractive arrangement of prepared food over the counter is desirable. The space requirement of 10 sq. feet per person is adequate. The dining hall and cafeteria is essential requirement when food is served to personnel, visitors and students also.
The food containers, trolley, trays and cutlery brought back from service area for cleaning. They are washed and sterilized and dried. The washing area will require a three-compartment sink; one for pre rinse, one for soaking and third one for washing. After washing and cleaning of the trolleys, these are parked in the trolley bay.
In decentralized system, every ward must have garbage bins of adequate size they are emptied daily, preferably after the last meal. Proper inspection of garbage is essential for the control of wastage of food.
Floors must be of concrete or tile, easily washable and non slippery. Drainage system is a basic requirement to prevent blockage and trapping of water on the dishwashing area. The drainage points must be provided with metal gauge.
The kitchen must be provided with exhausts, for exhaustion of smoke and greasy material from the kitchen.
The kitchen and dining hall must be provided with the air curtains for control of flies and other nuisances.
It should be so planned as to make maximum use of day light. Proper lighting must be available at food preparation and processing area for occupational safety point of view. The light of 10 feet candle is adequate.
For cleanliness of the dietary services only clean and healthy employees should be permitted to cook.
They should not be allowed to enter in their routine daily wares, or street clothes. They should be asked to take shower bath, clean hands carefully, trim nail, use cap, masks and all preventive measures to maintain good kitchen hygiene. They should be provided clean uniform and with a strict dress code.
The requirement for employees will be:
Separate electricity supply and meters for dietary department for calculating cost. Telephone and intercom facility between steward, dietician and kitchen. Fire fighting equipment’s to prevent fire hazards.
The department should be under the control of Chief Dietician, who will be responsible for management of the dietary services of the hospital. As per the recommendation of Mudaliar Committee a qualified dietician should be employed in all hospitals having more than 20 beds.
Today’s kitchens care not only labour intensive but the equipment’s also play very important role in the dietary services. The equipment’s save time and energy; so these are responsible to a great extent for efficiency in the department. With the advent of new technology, the modern kitchen is highly dependent upon the sophisticated equipment. The various equipment’s are being enumerated as under:
Nutritionists/dieticians are responsible for maintaining/ upgrading the nutritional status of inpatients, advice the OPD patients to facilitate their medical treatment being given and help in speedy recovery since no medicine can be effective to its capacity if nutritional status is poor. Disease specific diets and feeds need to be carefully prepared, administered and compliance is noted along with the effect on improving overall condition of patient during his hospital stay. A workman is never complete without his tools. An institute’s nutrition department must be armed with latest tools to access the nutritional status and carry out clinical studies with perfection. Special training on ‘how to use these equipment’s should be imparted to the dietetics students so that the work can be carried out with efficiency. For this, help may be taken from the experts of the growth lab, which is usually situated in the paediatrics department of the hospital, since correct assessment goes a long way to improve medical outcomes. Equipment such as height scale/bed scales, electronic weighing scale/bed scales, basal metabolic rate (BMR) and body mass index (BMI) calculator, body fat analyser, lean body mass analyser, Harpenden Skinfold Calliper, metallic inch tapes, etc. should be an essential part so that proper clinical services along with state-of-the-art research and training can be carried out for the patients any premier medical institute.
This is an important part of the nutrition wing in a medical research institute. Students are admitted for internship as well as short-term attachment courses varying from 3 to 9 months. It involves theoretical and practical application of the knowledge in ward and OPDs. Students are required to take up cases under the guidance of nutrition officers and present them before completion of their training
It would be desirable that the nutrition department has tie-ups with biochemistry lab and growth lab of the institute so that some micro and macronutrient tests like urinary urea protein to access dietary protein intake, serum vitamins and mineral levels, trace element levels, which are not sometimes routine tests for the patient, can be conducted for case studies and other research work. Growth lab can facilitate in anthropometric measurements or in training the students to use the tools for the same. All project work done by the medical faculty must make nutrition intervention an important part, since nutrition forms the backbone for favourable medical outcomes. Only thing is that this needs to be realised by the medical fraternity!
It should be made mandatory that the nutrition department has community services in their agenda, since no matter what you ‘Google down from internet for community preaching, imparting theory after practically experiencing it can never take a beating. Separate days for community services should be laid out, while some staff should be back there for clinical services.
It is one of the major areas of meal service in a medical research institute, since such type of institutes invite a lot many delegates and foreign faculty for their conferences, convocations, examinations, meetings, research agendas and what not. Usually, it is the responsibility of dietetics/nutrition department of the institute to cater to all the institute hospitality. In wake of huge gatherings, it might be that the caterers from outside are roped in, but still the onus of how good or bad the result was lies on the dietetics department. Many a times it leads to a clash between the standard of patient meal and institute’s hospitality. To be true, the patient meal always takes a back seat. It is not that it is not been taken care of, but to participate in a race and to participate to win differs a lot. The spirit to win is diverted towards hospitality and meal service in hospital caters to only participation at such times! This happens because all the best cooks and bearers are given the job to dish out various delicacies and serve them with utmost care. Monitoring of clinical side of the hospital also takes a backseat. It is like serving a guest who has come to your home with your best-possible capabilities, even at the cost of your health! The best-suited way might be to bifurcate the clinical and hospitality side of the institute. This job is best suited for hotel management pass outs. The able candidates from there should be recruited for a separate wing of hospitality for the institute. They can use their creative ideas and take hospitality to the next level. Nutritionists/dieticians should be made to concentrate on clinical and research side of the hospital meals so that important breakthroughs in therapeutic nutrition may be reached to take the nutrition in a hospital to the next level!
Management of dietetics unit of a hospital requires concerted and dedicated efforts by all members of the team to ensure that quality food reaches the patients of the hospital. It involves multiple components of management apart from cooking and serving food to ensure smooth functioning of the unit all the times.
Managing of dietetics unit can only be possible if technical knowhow, business administration knowledge, expertise in nutrition knowledge, art and craft of cooking, and presentation is blended into one for a perfect mixture called dietetics unit of hospital. Awareness about technical knowhow becomes a basic need in planning the very infrastructure of the dietetics unit along with the machinery and the equipment required; business administration skills are required right from procurement of raw material, be it perishable or non-perishable food items or any other material like packaging material, etc. to their storage, usage and accountability. In addition, handling manpower and maintenance and upgradation of all equipment’s definitely requires this skill. Expertise in nutrition along with art of making and presentation of diet of course forms the backbone of the dietetics unit, since this is the main thing that needs to be delivered from here to the patients in form of nutritious therapeutic diet as well as diet counselling sessions to support their medical therapy and enhance quality of life.
A qualified catering manager heads the catering services unit in coordination with the catering manger. He is responsible for the preparation and serving of therapeutic and special diets for patients as per the menu orders issued by the dietitian. Normal diets are also prepared and served those who require normal diet during hospitalization. The catering service unit operates food, beverages, and snack service to staff, students and visitors also, which is called as “cafeteria service”.
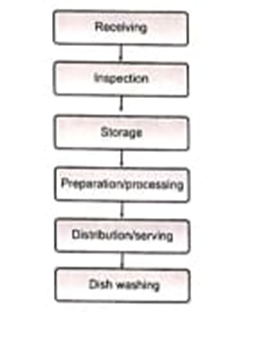
Procedures include checking delivered materials as to correct quantity, and package condition; checking scales accuracy; correct storage of different foods; opening cans, and other containers; weighing ingredients; boiling rice, vegetables meat and other food materials; and preparing various food items and special diets. They include carving meat; assembling patients’ meal trays; transporting meals to wards; storing unused cooked food; washing and sanitizing equipment; washing and sanitizing floors; evaluating and controlling plate-waste.
Rules include perishable items refrigerated promptly on delivery; odour-absorbing items stored away from odour-emitting items; special diet orders in writing by physicians; food during preparation tasted with spoon and not fingers; “holding” meals for patients delayed, such as by extended treatments; cooked foods refrigerated promptly in clean, covered, and shallow containers; plate-left-over meal items not re-served; and workers with infections prohibited from being on duty.
Facilities and Space Requirements:
The hospital cafeteria provides services for the hospital staff, visitors, and even ambulatory patients. It is usually near the food preparation area. The working time of the cafeteria is normally from morning to the closure of visiting hours for economic feasibility. Self-service pattern is advisable by delivery through service counters. Sufficient tables and chairs are desirable. Hand wash and bins for disposable plates and cups are mandatory.
The following questions are to be answered to control and establish good performance: